
Cardiologists today have a wide arsenal of methods for surgical treatment of coronary heart disease. Prior to the advent of intravascular treatment, the only surgical treatment was coronary artery bypass grafting (creating a shunt to bypass a narrowed area of a blood vessel using one's own veins or arteries). Today, many patients are able to avoid open heart surgery through the use of effective minimally invasive techniques, one of which is coronary stenting (coronary artery arthroplasty).
transluminal coronary angioplasty. This name reflects the essence of the procedure:
Transluminal - access to the vessels of the heart is made without incision, using a puncture through the skin, arteries located on the thigh or forearm; delivery of the necessary devices is carried out inside the lumen of the vessel.
Coronary - treatment of coronary (heart-feeding) vessels.
Angioplasty - increasing the inner diameter of the vessel with a special balloon, also known as - "Ballooning".
The concept of expanding the affected areas of the vessel with a certain framework 40 years ago was proposed by Charles Dotter. The development of the method was long, the first operation on this technology was performed only in 1986. And only in 1993 the effectiveness of the stenting method was proved to restore the patency of the coronary artery and keep it in a new state for a long time.
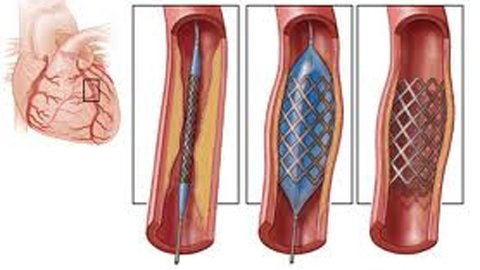
The stent is a thin metal mesh tube that is inflated by a special balloon. It is introduced into the damaged area of the vessel and, expanding, pressed into the vessel wall, increases its lumen. This restores the blood supply to the heart.
Coronary angiography determines the nature, location, degree of narrowing of the coronary artery and the size of the stent to restore the lumen of the artery.
Stenting is performed in the same X-ray. operating room, as well as coronary angiography, without skin incisions, under local anesthesia. Stenting lasts, as a rule, 20-30 minutes at full contact of the doctor with the patient. The doctor asks the patient how he is feeling, sometimes offering to hold his breath or take a deep breath. All the necessary parameters are monitored: ECG, blood pressure, invasive pressure, oxygen saturation and more.

A special catheter is inserted through a vessel on the thigh or arm at the mouth of the coronary artery, through which a thin metal conductor is made under control on the monitor. With the help of a conductor to the narrowed area of the vessel is a special balloon, the appropriate size in a compressed state. The stent is also mounted on the balloon in a compressed state. The stent is flexible and elastic, made of high-tech materials (alloys of precious metals), inert to body tissues and able to take the form of a vessel. The inserted balloon on the conductor is inflated, the stent expands and is pressed into the inner wall of the vessel. Control angiography is performed to determine the degree of stent opening. If necessary, the balloon is inflated several times, or a special high-pressure balloon is inflated to fully open the stent. The pressure can reach 16-18 atmospheres. The balloon is then inflated and removed from the artery along with the conductive catheter. The stent remains and preserves the lumen of the vessel. Depending on the size of the vessel, there may be one or more stents.
Usually the results of the operation are good. The operation itself is relatively safe and the risk of complications is minimal. Allergy to a contrast agent and stent thrombosis are extremely rare. Sometimes a hematoma is possible at the site of the artery puncture. (Link to video - Khokhlov's interview, where he talks about the minimum of possible complications) To prevent complications, the patient remains in the intensive care unit. But in a few days (after the puncture site heals) he is discharged home. Restrictions are usually removed after that, the patient returns to a normal active life, follows only simple recommendations for taking certain medications and is observed by a doctor at the place of residence.

Bloodlessness and apparent simplicity of operation, short postoperative period and efficiency of coronary stenting make it modern and a popular method of dealing with coronary heart disease.
Unlike coronary artery bypass surgery, which uses deep anesthesia, a sternum incision and an artificial circulation, the stenting procedure takes about 30 minutes (there is a possibility of repeated use in cases of progression of atherosclerosis), has a short postoperative period and has virtually no complications, and the patient is in fulland consciousness.

The method of stenting is progressively evolving and today there are opportunities for stenting not only coronary arteries, but also the arteries of the lower extremities, aorta, carotid arteries, cerebral arteries and shunts after coronary artery bypass grafting. Currently, new generations of stents with a drug coating on them are actively used to prevent excessive tissue growth at the site of stent implantation. The use of coated stents reduced the risk of re-narrowing of the vessel at the site of stent implantation from 30% to 3%. Stents capable of resorption 6 months after implantation are being put into practice. These stents are made of organic materials and have an advantage over metal. Increasingly, puncture of the arteries on the wrist is used, or special devices for suturing the artery after stenting, which further shortens the postoperative period and virtually eliminates complications.
However, it should be remembered that even the most modern cardiac surgery techniques are not eliminate the need for prevention and care for the health of your heart. Age-appropriate physical activity, age-appropriate physical activity, vitamin- and micronutrient-restricted diets with cholesterol-containing foods, smoking cessation, positive emotions, and stress-tolerance are concepts that never lose their relevance.
| Doctor | Name | Specialization | Reception time (Sunday) |
|---|---|---|---|
 |
Kamyanchenko Vyacheslav Nikolaevich | Anesthesiology, Cardiology | - |